There is horror and there is awe and smack dab in between the two there is desire.
What do I do with my desire? Often, I don’t know what to do with it. Just as often, I’m not sure that I am even close to understanding it. We are never more adrift, confused, fucked, misled, and dishonest (with ourselves and others—intentionally or not at all!), than we are in the domain of desire.
Yet desire is relentless. No matter where we flee, it overtakes us. No matter how we fortify ourselves, it overwhelms us. It is the drip, drip, drip of a slow leak; it is the gush and rush of a flood. It is the fifty to seventy percent of you that is water. What the Psalmist says of his god, we can say of desire:
Where can I go from your spirit? Or where can I flee from your presence? If I ascend to heaven, you are there; if I make my bed in Sheol, you are there. If I take the wings of the morning and settle at the farthest limits of the sea, even there your hand shall lead me, and your right hand shall hold me fast. (NRSVUE)
We want and we want and we want, and we think we know what we want and sometimes we do and sometimes we don’t and, either way, our wanting never wanes for long. Respite! We seek it wherever we might find it—microdosing dopamine on social media, binge-drinking on weekends, shopping and working and working and travelling and extracurriculars and adrenaline rushes and sports and hobbies and working and sex and working—because the relentlessness of desire causes us to suffer.
Or is it the relentlessness of suffering that causes us to desire? If I got what I want, I say to myself, I would not suffer—not like this, not this way. And yet, time after time, I find that I get what I want and my suffering persists. Perhaps it shifts slight but, at its core, it feels the same. It hurts and discomfits me just as much as it did before.
Two things offer us succour, but from seemingly opposite ends of an experiential spectrum.
Well, my “reviews in review” are different this year as I stopped posting my monthly book, film, and documentary reviews. However, I still wanted to do a year-end roundup highlighting the “best of the best” and the “worst of the worst.” It helps me keep track of where I’ve come from and where I’m hoping to go in the new year. Bien. Here we go.
In 2025, I read 165 books, watched 99 movies, and watched and additional 52 documentaries. That’s a lot, even for me (I should really develop more of a social life…)! Next year, for the first time in a very long time, I think I may spend less time reading books that are new to me and, instead, go back and do a more sustained engagement with texts or authors that have left a strong impression upon me. I’m thinking about re-reading all of W. G. Sebald, for example, and seeing if some kind of reflection arises from that. Or, to pick another example, going back through the affect theory material I’ve read (along with some of the psychology stuff I’ve read from the likes of Bollas, Phillips, and Leader) to see what happens if I try to weave all that together in a way that excites me. That sort of thing. We shall see. Onwards, then, to the “best of the best” and the “worst of the worst.”
The Books
A few general observations. I read a significant amount of fiction this year and I’m quite happy with that. I also made a point of making sure that 90% of the fiction I read was by female-identified authors and I’m glad I met that goal. I’ve been making a point to try and read more women authors for a few years now—in part to try and counter the prominence of “the great men of literature” that dominate the public discourse and, in part, because I find most of my favourite authors, the ones who resonate most with me personally, are women (Drndić, Heti, Lockwood, Solà, all come immediately to mind).
In fiction, I also continue to try and read authors from around the world, although I think I read a fair bit more English-based authors this year than I have in previous years. That’s okay. Next year, I intend to try and be more deliberate in looking up authors from countries I have not yet experienced through literature. Asia and Africa are, of course, the least represented continents in my reading list. I’m torn between exploring that (massive!) options and going back to read more books by authors I know I will always enjoy. We’ll see what happens.
My engagement with various forms of writing continues to ebb and flow. I still find myself very interested to read texts written by psychoanalysts, affect theorists, and authors writing in the “science and nature” category. Reading in these areas fills me with curiosity and wonder—critical resources for living the kind of life I desire to live—and make me ask questions I have never considered before and see things in ways I have never seen before. Additionally, the category I have termed “subaltern spiritualities” is one that I have very much enjoyed exploring and I intend to read a lot more in that category next year. It inspires good thinking, creativity, curiosity, playfulness, and what-the-fuckness in me. It has also been a personal avenue back to engaging with the “spiritual” side of life which has been life-giving for me (as it is, in a multitude of ways, for so many subaltern groups pursuing things like liberation, decolonization, and emancipation). In 2025, I intend to focus more on Quimbanda, Vodou, and Igbe, along with Nordic conceptions of fate and Ørlǫg.
Some categories hold less and less interest to me. In particular, reading in the areas of economics and also in several critical theory categories—particularly as they pertain to my own area of work within, against outside of the non-profit industrial complex—has waned significantly. Over the last several years, I did a sustained study of neoliberalism. For most of my adult life, I have also been reading texts that pertain to how oppression operates in relation to the mass production of things like poverty, immiseration, and homelessness. I think I have a thorough understanding of these matters now and further reading—apart from a few texts here and there—mostly just depresses me and leaves me feeling increasingly hopeless (all these texts remind me of a quote Mark Fisher attributes to both Fredric Jameson and Slavoj Žižek: “it’s easier to imagine the end of the world than the end of capitalism”). In fact, I have a massive amount of notes pertaining to these things for a text I intended to write about neoliberalism, homelessness, and the various models of resistance that arise within communities of frontline workers and others (based in part upon my own sustained engagement in various communities of solidarity, resistance and liberation, over the years), but I find the whole matter too disheartening to dwell on in any sort of sustained manner. That book may never come to be and I’m okay with that. I’m getting old. I have fought a long fight for most of my life. Now, I wish to focus less on our enemies and more on what I love and, in fact, what gives me pleasure.
The Best of the Best
As always, it is difficult to pick the “best of the best” books read in 2025 and the following is entirely subjective, based upon my own personal aesthetics, and what I happen to be experiencing at the time of reading. With that in mind, the book that stood out to me as my favourite book of 2025 is No One Is Talking About This by Patricia Lockwood.
[On October 22, 2025, I was invited to participate in a “Story Day” event in Toronto. This is an annual event organized by Erinn Oxford and the team at The Dale. I am very grateful to have had the opportunity to participate. This year’s theme was “Accessibility.” Below is the transcript of what I shared.]
Introduction: Hello, my name is Dan and I am a Canadian settler of Dutch, Scottish, and Irish descent. I was born in Anishinaabe, Haudenosaunee, Lenape, and Chonnonton territory, in a place now referred to as London, and I continue to reside there with my children.
Tonight, we have gathered to share stories about accessibility. To me, this inevitably raises the question of barriers, things we construct—as organizations, cultures, and nations—that make certain things inaccessible to certain people. Storying accessibility raises the issue of oppression—and how we go about collectively liberating ourselves from it.
However, oppression and its multitudinous barriers are designed to be hard to see if you are a person who benefits from oppression. The more you benefit from oppression, the harder it is for you to see the ways in which others have radically different experiences of the very same people, places, and things as you. Thus, learning to see is essential to learning to be free. The first of the two short stories I will tell provides one example of that kind of learning.
[I recently completed Miriam Toew’s latest book, A Truce That Is Not Peace (2025). I found it deeply moving. It prompted me to write the following reflection and I deliberately wrote it in a way that harmonizes with the voice Toews deploys in the book. Be warned: suicide is a prominent theme in what follows. I did consult with my brother prior to sharing this publicly and am doing so with his permission.]
Wittgenstein famously concluded his Tractatus by saying: Wovon man nicht sprechen kann, darüber muß man schweigen [Whereof one cannot speak, thereof one must remain silent].” But poets and novelists have a different idea of what is speakable, what is not, and what other ways we might have of drawing closer to the unspeakable with words.
Then, later in life, Wittgenstein offered this corrective to his younger self: for heaven’s sake, don’t be afraid of talking nonsense. But you must pay attention to your nonsense.
Miriam Toews is a writer who pays close attention to her nonsense.
“TaranTula” by Christina Sporrong (photo by Doug MacCash/NOLA.com)
Once, in the world of the insects, bugs, and creepy-crawlies, there was a spider who wanted more.
“This is not the life for me,” the spider said to himself. “It is not enough for me to sometimes have what I need, sometimes have a little extra, and sometimes not quite have enough. I deserve so much more. I should be able to have a fly for breakfast, a fly for lunch, and a fly for dinner every day. I should be able to have a fly—no, two or three flies!—as a midnight snack if I’m feeling peckish.”
“I am not like the other bugs,” the spider told himself. “I don’t suck on dirt like a worm, or chew on wood like an ant, or sip from flowers like a butterfly. My palette is more refined! I dine on the juices of those who are still alive. And my technological innovation is nonpareil. I design webs based on precise mathematical models and objective precision. I take empty space and develop it, weaving my web hither and thither, so that it becomes something with real value. Really, I deserve to have whole storerooms full of flies.”
“Yes,” the spider concluded, “I should have one billion flies.”
His eyes full of his own potential, the spider began to weave a web. The web he wove grew larger and larger. Soon, he was having a fly for breakfast, a fly for lunch, and a fly for dinner every day. But the more he ate, the hungrier he became. He built his web larger and then he was able to have not just one but two and then three flies as a midnight snack.
The other insects, bugs, and creepy-crawlies started talking amongst themselves.
“Things are really getting out of hand here,” said the flies.
“Oh, I don’t know about that,” said the rolly-pollies.
“No, for real, they are,” said the flies.
“I don’t see any kind of problem,” said the termites.
“You will soon,” said the flies.
“I don’t know about that,” said the sole Luna Moth.
Meanwhile, the spider was still feeling a little peckish.
He re-examined his web. Some parts were breaking down. It was a lot of real estate for one spider to maintain. Some parts were derelict and abandoned. Some parts had holes. He went to work on reinforcing his web. Soon, he was bringing in all kinds of bugs. Some days, he would eat half a fly before dining on the eyes of a roll-polly, and the liquified organs of a termite. He began tossing half-eaten bodies away.
“This is the life!” he thought to himself, while scratching his thorax with the proboscis of the Luna Moth. “I’m not a ‘eat stale leftovers’ kind of guy.”
The other insects, bugs, and creepy-crawlies had a meeting.
“Things are getting out of hand here!” said the rolly-pollies.
“I told you so,” said the flies.
“This is a real problem,” the termites confirmed.
The Luna Moth said nothing because she was dead. Well, not quite all the way dead but suspended in a near-death state in the spiderweb, where the spider would go to “nip a sip” from her abdomen when he felt like he deserved a special treat. Which was most of the time.
“We should probably have a meeting with the spider,” said the rolly-pollies.
“I don’t think that’s a good idea,” said the flies.
“I’m sure he’s a reasonable guy,” said the termites.
“Don’t make me say ‘I told you so’ again,” said the flies.
The next day, the bugs all met with the spider to express their concerns.
“Look,” they said to the spider, “we understand that everyone needs to eat. We all give and we all take away. We all treat some others as food and are, in turn, food for some others. Life cycles. Some forms absorb some others forms which are, in turn, absorbed by other forms. And so on. You don’t need to watch The Lion King to understand this.”
“Watch the what?” the spider said.
“Never mind,” said the other bugs. “The point is that while life and death are all a part of living and dying, and while we all contribute to both of those things, your shit has gotten really out of hand.”
“You really think so?”
“Well, you are scratching yourself with part of my friend’s face,” the bugs pointed out. “You didn’t have to bring that to this meeting.”
“Fair,” said the spider, trying to casually tuck the Luna Moth’s proboscis away.
“Also, I think you have part of Derek still stuck between your fangs,” said the termites.
“Ew!” said the flies.
The spider wiped his fangs.
“If you don’t change your behaviours,” said the flies and the rolly-pollies and the termites, “then we will unite ourselves against you. We will chew down any plant you use as an anchor. We will gnaw through any wood you use as a base. We will drop sand into your webbing. We will make your life a living hell and you will starve to death. By grasping for everything, you will end up with nothing.”
The spider did one of those blinks where all eight eyes blink at once. (“Creeeeeeepy,” whispered the flies.) He rubbed his fangs and reached for the proboscis to scratch his itch before remembering where he was.
“Maybe we got off on the wrong pedipalp,” the spider said. “I’m willing to concede that there may have been some design flaws in my web. I didn’t catch and eat every fly or bug or creepy-crawly that flew or crawled or stumbled into it. There are definitely some holes, and gaps, and blind-spots. Some parts that aren’t being put to best use.”
“I’m not sure we’re talking about the same thing here,” said the flies.
“Shhh, let him finish,” said the termites.
“So rude,” said the rolly-pollies.
“So, what I think we should do,” the spider continued, “is all work together to solve this problem.”
“Great idea,” said the termites.
“What we really need,” the spider said gaining momentum, “is a consultation group composed of flies who have lived and living experience of being caught in the web!”
“Yeah!” said the rolly-pollies.
“Um—” said the flies.
“That way,” the spider said growing in majesty with every word, “we could draw on their expertise in order to design a web that is truly inclusive of everyone!”
“Yippee!” said the termites.
“Put out an RFP!” said the rolly-pollies.
“I though we wanted a less inclusive web?” the flies said. But they buzzed too softly and were drowned out by the swell of applause.
And so, the working groups were worked, the consultation groups were consulted, the advisory groups were advised, the committees were committed and the sub-committees were sub-committed and a new web was built. One year later, the bugs came together to review the progress.
“According to the stats I have gathered from my, um, ‘centralized intake’,” the spider said wiping his fangs, “this has been our most successful year so far.”
“Really?” said the termites.
“Really!” the spider said.
“It’s kind of weird that the flies aren’t here,” said the rolly-pollies.
“Totally,” said the spider, trying to muffle a belch.
“Yeah, they usually want to say ‘I told you so’ or something at these meetings,” the rolly-pollies continued.
“I always found them to be real downers,” said the termites.
“Yeah,” the spider said. “Besides, you catch more flies with honey than with vinegar.”
“Huh?” said the termites and the rolly-pollies.
“Oh, it’s just a silly little saying,” said the spider.
“Oh, hahaha,” laughed the termites and the rolly-pollies.
“Ready for the next RFP?” asked the spider.
The bugs applauded. Eventually, the spider ate them all. And then he died, too.
I don’t want a seat at the table. The table is full of oppressors. I want a blanket and a pillow down by the ocean. I want to rest. Tricia Hersey, Rest Is Resistance
5: The Political is Personal (continued from previous post)
Accepting the usefulness and validity of the conclusions drawn in Part 1, means that we have to look at more than local networks, structures, aggregate data pools, and “biopsychosocial indicators of health”—we also have to look at the decisions made and the actions taken by specific organizations and specific individuals. Oppression persists not simply because it is structured into society but because there are specific parties who create those structures, who maintain and reinforce them when they are challenged, who profit from them, and who sign the papers that ensure many of us will die so that a very few of us can expand the assets held in their portfolios. To riff on the quote attributed to Utah Phillips, the forcibly impoverished and dispossessed aren’t dying, they are being killed—and those doing the killing have names and addresses.
But, wait, we know who these people are in our local municipality. In fact, we’ve personally interacted with many of them. Especially during the “systems-wide health and homelessness response” the City of London initiated when a coalition of frontline workers (#TheForgotten519) successfully challenged the City’s power, their ability to control the public narrative, and the priorities they were setting.
We met representatives and personal hoarders of vast amounts of (stolen) land and wealth (like real estate developers, the heads of local “Business Improvement Areas”, and bankers);
We know many of the municipalbureaucrats who manufacture homelessness and death via legal technicalities, bylaw amendments, selective enforcement protocols, and budget choices;
We know many of the non-profit bosses who are happy to follow the money and engage in increasingly punitive actions against the most vulnerable people they claim to serve in order to satisfy the demands of the rich (White benevolence was well-represented, as was Christianity);
We also know the doctors and healthcare professionals as well as CEOs of health institutions who reject harm reduction, who make mad money from the Opioid Agonist Treatment industry, and who generally hate impoverished people whose access to healthcare has been criminalized (I vividly remember the then-CEO of the hospital asking if we really needed to implement anti-oppression practices because, “everybody can just be nice to each other”—when she was speaking, I was thinking about everybody I knew who had died from stupid causes, like easily-treatable blood infections, because they were kicked out of the hospital [for self-medicating their own pain because the hospital wouldn’t give them pain meds] then beaten by security guards and told to never return).
They people responsible for manufacturing homelessness and producing premature and preventable deaths are well-represented the table. They chair our working groups. They control most of our sector’s funding. They set the priorities and define success for most organizations. They control the narrative that is fed to the public.
[O]verseers give you a superior smile, but death lurks in their hearts. Martin Buber, I and Thou.
1: Whither Liberalism?
To make society… happy… it is requisite that great numbers… should be ignorant as well as poor. Bernard de Mandeville, The Fable of the Bees
In his counter-history of liberalism, Domenico Losurdo asks how it is possible that the Europeans and Euro-Americans who spoke most vehemently about the freedom and rights of the individual at the dawning of what we call liberalism, were also the people who defended, unto the death, their right to keep Black people as chattel slaves and their right to engage in genocide against Indigenous peoples in various colonial occupations. The discourse of freedom is applied to massive acts of dispossession and violence. What is going on here? what exactly, Losurdo asks, is “Liberalism”?
Essentially, Losurdo argues, Liberalism is a doctrine pertaining to a very specific form of freedom. This freedom was declared to be the inherent right of White men with property and it manifested in two primary ways:
It was freedom from the tyranny of those who sought to rule over them
notably, the aristocracy, the agents of the church, and also the governmental agents and growing legal codes of nascent nation states;
It was freedom to engage as despotic rulers over subaltern people
who they considered their property (largely Black folx—think racism);
who they considered subhuman and part of nature to be subdued or exterminated by whatever level of violence they deemed desirable (largely Indigenous folx—think colonialism);
AND who they considered uncivilized, immoral, idel, criminal, and frequently irredeemable even with the metropole or the heart of the empire (largely the rural and urban poor—think classism).
Thus, the Liberal is positioned between, and distinguished from, two other parties:
The Conservative who harkens back to more traditional forms of tyranny which were frequently antagonistic to the bourgeois, middleclass and small property owners;
The Radical who believes that freedom from tyranny also applies to subalterns, like Black folx in Haiti singing La Marseillaise while going into battle with the French
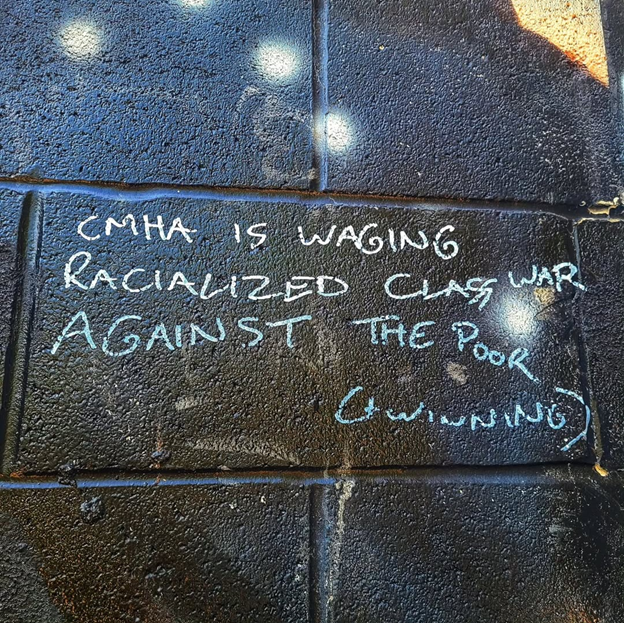
Thus, as many scholars have argued, the rise of Liberalism was a part and parcel of the rise of Capitalism. The two have been solidly intertwined over the course of their shared history. However, as autocratic imperialism and various forms of fascism have demonstrated, Capitalism can thrive without Liberalism, Liberalism, however, cannot thrive without Capitalism. Why? Because Liberalism is the political ideology of private property owners. It arose to prominence when the bourgeoisie betrayed the proletariat and the capitalists replaced the aristocrats. It has stayed true to that racialized class war on two fronts to this day.
Thus, the freedom praised by Liberalism is always the freedom of the property-hoarder over against both the dispossessed and any other authorities who might wish to interfere with the ability of the property-hoarders to take and privatize and hoard ever more.
1. Alcohol is Fun and You Can Still Be Responsible and Have Fun with It
With legal drugs (i.e., “controlled substances”) we understand that recreational, pleasure-inducing use is totally fine. In fact, such use for the sole sake of enjoying the feelings or affects induced by the drug is encouraged—not only by legal drug-producers and -pushers like the companies that craft, advertise, sell, or otherwise profit from people taking those drugs, but also by various drug-user cultures that are normalized within our society.
Thus, for example, all kinds of alcohol are marketed to all kinds of groups and various cultures arise in relation to various brands. If someone wants alcohol that comes from grain malt mash, or grapes, or distilled spirits, that says something about who they aspire to be. Working men drink cheap, patriotic beer. Wine moms drink wine. Hipsters drink IPAs. Rich men and boss women drink Scotch. People who hunt ducks drink Bourbon. I’m sure you can add other drug-use cultures to this list.
All of this occurs even though we are aware that these drugs can be dangerous and harmful. This is why they are controlled substances. Bars are supervised consumption sites for alcohol and they are widely available and easily accessible; businesses are required to ensure that they do not sell alcohol to those who are below the legal drinking age; people are legally forbidden from drunk-driving; alcohol products not intended for consumption aren’t sold alongside of Sherry, and so on.
However, despite these various controls, harms still occur. Yet this does not lead to full criminalization or a total ban on the pleasurable use of these substances—such things have been tried in the past (the USA tried this with alcohol from 1920 to 1933), but these efforts always end disastrously and the harms caused by criminalization are vastly greater than the harms that persist whenharm reduction is applied to alcoholand other substances and their use is both encouraged and regulated (countries like Switzerland and Portugal, as well as various studies done in Canada, Australia, the US, Germany, France, and a host of other countries demonstrate that this conclusion basically applies to all controlled substances that people also use recreationally). However, alcohol is the most widely available and taken-for-granted controlled substance. Therefore, because drinking alcohol can be a fun but not risk-free activity, the saying “enjoy responsibly” is ubiquitous in the drug-user culture associated with alcohol.
Observe: Nobody is saying that you shouldn’t drink for fun. They’re just saying that, when you do drink, you should try to do that in ways that don’t hurt yourself or others. Importantly, we’ve structured our society in such a way so as to institutionalize and legalize safer forms of controlled substance use (for this substance).
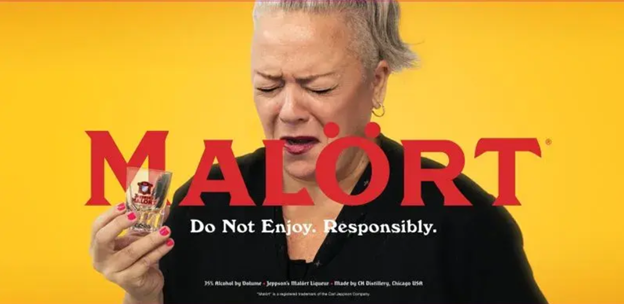
Drug users whose drug of choice is alcohol have a good deal of fun with this responsibility-oriented sloganeering. The Chicago-based company Malört plays with the observation that the bitters they produce actually taste, well, really fucking bitter and really fucking gross and so they created the following ad:
In fact, the whole injunction to drink “responsibly” is an easy target for all kinds of jokes (especially after you’ve had a drink or two!). Here are a few examples:
And this one makes me lol:
There is also a brand of beer “devised by [a] wacky entrepreneur” (according to the Daily Mail) that allows you to drink as much as you want while still drinking ResponsiblyTM:
You get the idea: (a) people drink for fun; (b) they are supported with this via harm reduction methods that have been tried and found to be far superior to criminalization; (c) and people who drink often laugh at the discourse that urges “responsible use” because, hey, sometimes people just want to get fucked-up; (d) and, hey, it’s okay to laugh at other people’s notions of “responsibility” (especially given the ways in which neoliberalism uses individual “responsibilization” as a way of depoliticizing our understanding of our context and as a club to bludgeon the oppressed); (e) and, hey, nobody is being treated like a shit-stain on the community just because they joke about how “drinking responsibly” means using a coaster and not spilling their drink; (f) and, hey, having kids is hard fucking work and if you want to get together with other moms and cry-laugh about how the only thing that sustains you is alcohol while sipping a glass of White Zinfandel, that doesn’t mean you’re a bad mom and you can totally do that.
2. Taking Medication is a Less Fun Way to Do Drugs but Sometimes Meds Really Help
In light of this, it’s interesting to observe how well-intentioned advocates of harm reduction, decriminalization, and care for people who purchase, possess, or use controlled substances in ways that have been criminalized, don’t talk too much about how using these drugs can also be a really fun experience (I include myself in this critical observation and what I say here relates to what I wrote in my recent post, What Do We Talk About When We Talk About “Addiction”?, so I won’t repeat here what I said there). This is because of the ways in which people whose possession or consumption of drugs has been criminalized are frequently portrayed as irresponsible, immoral, vice-ridden, lazy, ne’er-do-wells. Consequently, when talking about drugs, these advocates (again, myself included) tend to talk about drugs as medications.
For many people who have been forcibly impoverished, abandoned, oppressed, and pushed-out, access to healthcare simply does not exist in the same ways that it does for upper-middleclass members of dominant populations. It’s not hard for university students to get Adderall (which, as Carl Hart shows, is both chemically and experientially all-but-completely indistinguishable from crystal methamphetamine). It’s not hard for rich families to get Ritalin for their kids with ADHD. When you have money, it’s not hard to find doctors who take your pain seriously, who aren’t overly concerned about what you do with your pills (heck, you probably went to school with a number of other folks who became doctors and have them in your peer group), and who are willing to put up with you during appointments when you are ill-tempered, grumpy, “hangry,” or just acting like a White Man in PublicTM.
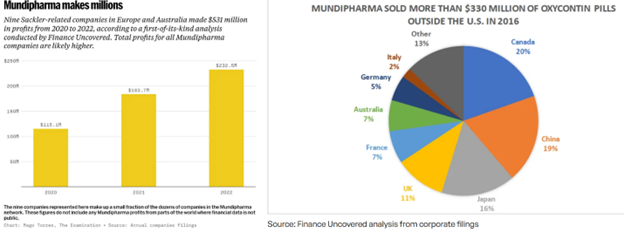
It also didn’t used to be hard for anyone to get opioids. Thanks to Purdue Pharma, the Sackler family, and tens of thousands of family doctors, a lot of low income folks, blue collar workers, and folks with various forms of temporary or chronic pain, could access opioids via their doctor or the Emergency Department at the local hospital. But the narrative shifted about opioids once it became clear that Oxycontin (remember Oxy80s? Heaven in a pill!) was very addictive and also rather more dangerous when it came to overdosing (Oxys, like the host of opioids that came before and after them, were first marketed as a low-risk, non-addictive alternative to other pain medications). So the regulators get more heavily involved and started threatening the doctors. The Sacklers were also dragged before the courts but they mostly got away with it and still have billions of dollars while amassing billions more—much of which comes from other companies they own outside of the USA selling both opioids and the drugs that are used to treat opioid addictions (and guess who holds the patent for Naloxone? Richard Sackler!).
Unfortunately (but not surprisingly, recalling that shit never flows upstream), going after doctors for “over-prescribing” just ended up producing a whole bunch of people who were physically and mentally reliant on opioids, often with chronic pain (and a higher sensitivity to pain due to regular opioid use—which was the drug-use schedule prescribed to them by their doctors) who could no longer access safe, pharmacy-grade medications. The very same doctors who created those chemical dependencies suddenly stopped providing the drugs.[1] As a result, people have needed to find alternative ways to medicate their pain, to address their withdrawal symptoms, and to try to and continue with wellness plans that, for many people, had worked just fine for years.
Knowing this, when people speak about “drug addicts,” or “people who use drugs,” or “substance abusers,” or “people who misuse substances,” advocates such as myself have been more inclined to replace all references to “drugs” and “substances” with the language of “meds” or “medications.” Hence, when it comes to the harms we associate with those drugs—like the mass number of deaths we associate with fentanyl and the so-called “opioid crisis”—comes down to having a safe supply—i.e., getting a guaranteed dosage of a guaranteed chemical cocktail from a reliable source (like a pharmacy) without any impurities mixed-in. Of course, a safe supply is what occurs when decriminalization occurs.
3. But Drugs Can Also Be Really Fun and That’s Great Too
Now, while I support this discourse, frequently employ it, and believe that it is an effective way to highlight biases that hide in plain sight based upon what we do and do not take for granted about different groups of people, I think it’s also important to emphasize that meds like opioids and other controlled substances can also be used recreationally and this is also totally fine! Sometimes the discourse of meds and its expansion into the domain of “illicit substance use” can end up being a form of respectability politics. Respectability politics, as Wikipedia handily summarizes it:
is a political strategy wherein members of a marginalized community will consciously abandon or punish controversial aspects of their cultural-political identity as a method of assimilating, achieving social mobility, and gaining the respect of the majority culture.
In this instance, the issue with respectability politics isn’t that it works to restore an inherent dignity and respect to certain drug users—that’s all well and good; rather, the issue is that this restorative work is done at the expense of other drug users, and is achieved by assimilating to oppressive cultural notions about what we are and are not allowed to do for fun, what the law is or is not allowed to tell us to do, and what it means to be responsible within a context where the notion of individual responsibility is commonly used as a tool for enforcing oppression. In fact, the picture below, while amusing (which is great—let’s be amused as we work through hard things, homies!), is also a very real presentation of one form of responsibility that applies to many people:
I was thinking about the joy of drugs and how advocates (like me) who talk about “meds” often inadvertently reinforce stigmas related to status quo values when I encountered the following piece of graffiti in a local stairwell (fetty = fentanyl):
Funny, right? But it also should make the passerby stop and wonder: “Hey, wait a minute, why do we take that stance with some substances that can be enjoyable-but-potentially-harmful but not others? Why do we draw the lines where we do? We do we take this slogan for granted when it comes to alcohol but not fentanyl?”
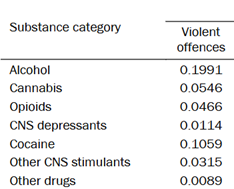
Well, large numbers of people are dying because they have accessed a toxic supply of fentanyl. As I have already argued here and elsewhere, this is because their access to this substance has been criminalized. However, the primary group of people who are fatally harmed by fetty-use are the fetty-users themselves. But, if we look again at alcohol-users, we cannot make the same argument. Not only are ~55% of fatal car accidents in Canada caused by impaired driving (with alcohol being the leading cause of impairment and recalling that the drunk driver is more likely to survive than others involved in the crash), but a 2021 report from Corrections Canada demonstrates that, of all drugs that people use, alcohol is the one that is most likely to be involved when violent crimes occur:
One could argue that the ubiquity of alcohol causes it to be over-represented here but: (a) we know that the harms it causes are less now that it is legal than when it was illegal; and (b) we don’t have to worry about something similar happening with opioids since a safe supply of fetty isn’t going to make you want to beat your spouse, crash your car into a family of four, or fight that annoying dude at the bar—it’s just gonna make you have one the best naps you’ve ever had in your life.[2]
Fetty, then, like a host of other drugs, is something that we should not stigmatize if it is used recreationally for the euphoria, relaxation, and sense of peace and well-being it offers (I mean, who doesn’t want to feel euphoric, relaxed, peaceful, and well?). However, because of the risks currently associated with its use (again, which are largely but not exclusively related to criminalization), the message to “enjoy responsibly” is an important one. By all means, enjoy the drug, but let’s try to be careful with it so that we do not harm ourselves or end up doing things we might regret because of how much we enjoy it (i.e., “do the drugs, don’t let the drugs do you”).
4. Unfortunately, It’s Hard to Enjoy Drugs When the Police Are Trying to Kill You for Doing Them
The problem, which should be apparent by now, is that criminalization, stigmatization, vilification, greed, cruelty, and the smug self-righteousness of those who are greedy and cruel, make it difficult for people to enjoy a lot of drugs responsibly. John Hardwick gets to the truth of this when he urges people not to do drugs because “if you do drugs you’ll go to prison, and drugs are really expensive in prison.”
In fact, we are currently witnessing a major assault upon people who enjoy drugs as supervised consumption sites across the province are being shut down and municipalities are shifting from talking about funding harm-reduction-based hubs to funding abstinence-based hubs (with many social services merrily going along with this in order to continue to lionize the funding). Due to this matter, and concerns about “open-air substance use,” massive increases to police budgets are being justified even though this means cutting other services to oppressed folx.
Thus, at the same time as safe, indoor spaces are being defunded and essentially banned via absurd regulatory strategies, the roaming gangs of cops in London (increasing from 2-4 officers to 6-8 officers with an embedded social worker from CMHATV) are becoming a much more regular presence on the street. This is a part of the law enforcement crackdown on “open air substance use.” Mostly, based on reports I have received from those who have nowhere safe to go in order to receive shelter, housing, and care, it sounds like the cops are telling people to “move along,” taking away their drugs, looking for reasons to detain them, and generally terrorizing them. The despair on the street right now is palpable.
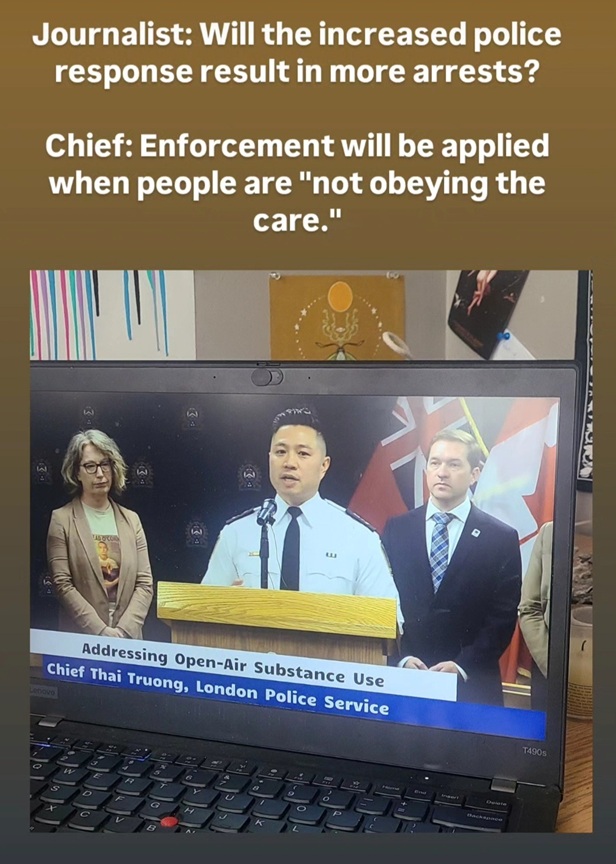
What’s remarkable is that all of this is being justified with the language of care. To be clear, it’s not remarkable that this language is being used—justifying oppression by calling it care has been around for ages (from White Saviours, to White Benevolence, to White Feminism, to White Social Working… wait, it’s almost as if there is a racialized and racializing element to oppression in our context…), and this tactic is alive and well today. What’s remarkable is that it still has any traction. People are still falling for this shit? That’s wild, because the ideology of care being administered by state-based violence workers leads to some truly outrageous and utterly laughable statements. For example, when asserting that increased policing is the solution to public drug use in our community, the chief of the local force had the following exchange with a journalist:
What a line! If you do not do as the police command you to do, you are “not obeying the care” and deserve to be punished with whatever amount of force the police deem necessary (I think even the chief, himself, realized the absurdity of his line which is why he kind of stuttered when he said it—he dove too deep into his own ideology and accidentally revealed how ridiculous it is)!
Thus, we can now add this line to a trifecta of fucking stupid things the police say when they brutalize community members:
And:
And then we can imagine the following:
That said, it’s also worth noting that we, as a community, feel compelled to do things like address “open-air substance use.” Why does it feel like “common sense” to all be talking about this? Why aren’t we looking at creating roaming gangs of cops and social workers to address “off-script Adderall-use at Western University,” or “cocaine-use in bars,” or “bowls full of every kind of drug imaginable at house parties in Old North”? If the police focused on any one of those areas, let alone all three, I’m absolutely certain they would bring in far greater amounts (both by weight and by dollar value) of drugs and I’m sure they would bring in higher level dealers. But the issue here really isn’t illicit drug use. It’s about helping the hoarders of (stolen) land and wealth move into neighbourhoods they deliberately impoverished so that those neighbourhoods can be gentrified, the already-impoverished folks can be forced to go elsewhere (“OBEY THE CARE!”), paying customers can move in and feel at home, and rich pricks can get a whole lot richer.
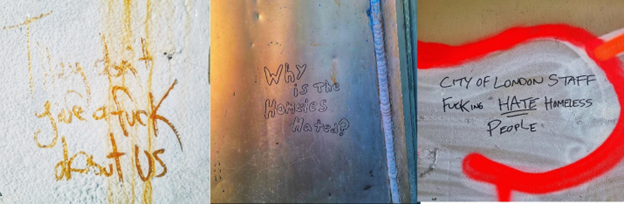
Therefore, when “care” looks like you getting your teeth kicked in by cops behind a dumpster because you were moving too slow while packing your things because you are in pain from withdrawing from meds you used to get from your doctor… when “care” looks like having to spend the weekend in cells and not being able to notify work and losing your job and then losing your housing because you couldn’t make rent, and then losing your kids because you lost your housing… when “care” looks like the outreach worker using their personal relationship with you as a form of “soft power” that enforces private property bylaws and moves you along (while the “hard power” of the police lingers in the background)… when “care” looks like not being able to receive medication for pain when you go into hospital with a spine infection that threatens your life, even though you have a considerable amount of pain but you’ve been flagged as a “pill chaser” and so you have to white-knuckle through the pain or self-discharge against the doctor’s orders… when “care” looks like being forced to go to places that are more and more removed from the general public and which afford a vulnerable person less and less safety and put you at greater risk for dying of an overdose from a toxic drug supply or being assaulted by a property owner who doesn’t want you in the woods by their house (homeless folks are assaulted by housed folks far more frequently than housed folks are assaulted by homeless folks)… well, it’s no wonder that graffiti like this is everywhere you look downtown:
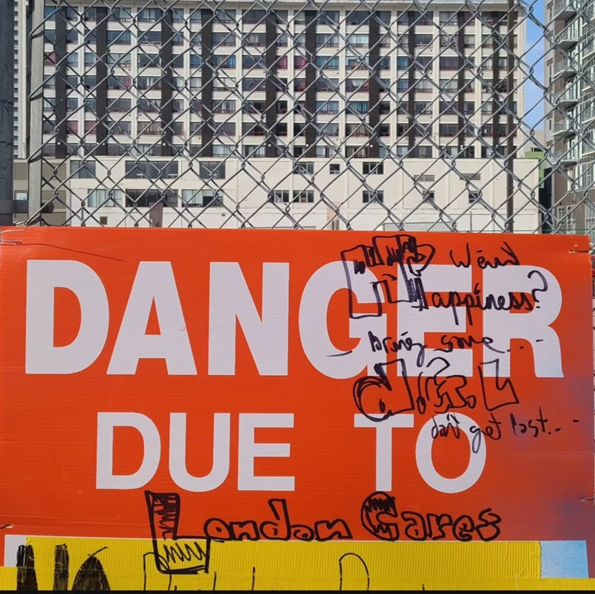
I expect to see people saying more things about CMHA now that they’re part of foot patrol (CMHA already exploited the Black Lives Matter movement to launch their other police-CMHA collaborations and increase their funding—as a result, they currently have 15 executives on the Sunshine List [i.e., 15 executives earning more than $100K of public sector funding dollars]—but their presence on the street has been exceedingly minimal so they don’t get mentioned much by wall-writers) but the main thing one sees over and over, given that the primary organization that has been doing Bylaw Enforcement work for the City is called “London CARES” is the statement: “London Doesn’t Care.” This is just one playful variation on that theme:
Not surprisingly, when the carceral state and the discourse of health and care blur into a single entity (a process that has gone hand-in-hand with the secularization of so-called Western nations), people can respond by having a laugh at the norms that brand them as deviant, the policies and regulations that exclude them, and the laws that kill them. Instead of taking on shame or guilt for being branded as deviant or as a failure, one can embrace that identity, play with it, and be proud of it. Just like alcohol-users can laugh at the idea of “enjoying responsibly,” so also other-drug-users can celebrate their use.
This happens all the time in pop culture (Car Seat Headrest sings, “Drugs are better with friends are better with drugs” and it’s very easy to sing along!), and everyone loves a good-hearted outlaw (or even just a badass, “I did it my way” motherfucker) and, yes, there really is jouissance to be found in doing what some ding-dong authority figure tells you not to do—especially when all that ding-dong authority figure really CARES about is making the poor fuck-off so that the rich can get more rich.
So, look, if this is care then, hey, I’m not obeying the care and I’m having the best time doing that.
5. Taking Drugs from Homeless People is Soul Murder—So Smoke ‘Em If You Got ‘Em!
In light of the above, I find myself returning yet again to Henrik Ibsen’s observation that depriving another person of the ability to experience joy in life is “soul murder.” I think soul murder is a term that captures what happens when people with money and power force other people into a joyless existence, defined by serial abandonment, unrelenting pain, and total immiseration, and culminating in premature, preventable, grinding, and altogether shitty deaths. In Toronto, the average age of death for homeless men is 50—for homeless women the average age of death is 36. This isn’t just soul murder, it’s soul genocide.
It seems, when it comes to forcibly impoverished folx, three things are held to be true. First, they don’t own enough goods to be good people (Bylaw Enforcement officers make sure of this by constantly going around to people’s tents when they’re not home and throwing all their belongings into the trash—a regular, everyday, normalized and accepted form of robbing the poor to satisfy the rich). Second, they are not permitted to be in shared public spaces (you have to be a paying customer or, if you’re on the sidewalk, you have to be at least a potentially paying customer for the businesses that are nearby and you should never be present in such a way that you cause the slightest discomfort to other potential paying customers which, alas, simply being poor in public does). Third, the forcibly impoverished are absolutely forbidden to have any kind of fun at all. So they are vilified, pushed out of everywhere, told that this is all their fault, and not permitted to have any kind of fun or spend their tiny bit of money on anything but the bare necessities (which, it turns out, the tiny bit of money they receive from social assistance doesn’t cover adequately), and if they dare to enjoy themselves, engage in recreational activities, have fun, spend a weekend getting high in a hotel room with a locked door, a shower, and clean bedding, they are branded as the absolute worst kind of sinner “living a high risk lifestyle” and ultimately deserving the premature, preventable, grinding, and shitty death that comes for them. That’s soul murder, too, and it culminates in literal, physical, bodily death.
In One Day, Everyone Will Have Always Been Against This, Omar El Akkad writes: “Forget pity. Forget the dead if you must, but at least fight against the theft of your soul.” He’s writing as an Egyptian-Canadian reckoning with the ongoing genocide in Palestine but I think his words also apply to the class war that is raging and escalating all around us everyday, across the globe and in the smallest local communities.
Getting high on fetty is a risky activity these days. It might kill you. But if enjoying that high and the pleasure it gives you is the only thing that is stopping the rich from stealing your soul—after they have already stolen your home and your land and your labour and your health and your children and your sense of belonging—then enjoy! And if you want to live, then try to enjoy “responsibly.” Try not to use alone. If possible, have Narcan and a sitter. If it’s available, use sterilized gear. Remember that smoking is a lot less risky than shooting (and, given all the deaths we’ve seen in the last few years, a lot of people have stopped shooting and only smoke now). And, with those things in mind, have the best time ever! You fucking deserve it.
[1] Although, N.B., as of 2023, there were still approximately 125,000,000 active opioid prescriptions dispensed in the USA. Similarly, in 2022 approximately 1 in 8 Canadians received an opioid script at some point. This highlights two important elements: (1) the class factor I have been addressing and the ease at which those who hoard (stolen) wealth are able to access these meds via the legally-mandated channels; and (2) the fact that only 10-20% of people who use any drug end up getting “addicted” (so way more people are taking opioids all the time and never getting “addicted” or ending up using them long-term).
[2] The legalization of cannabis is a good parallel here. Not that long ago, the government and the police were promoting the notion of “reefer madness” and, as they’ve done with innumerable other substances, arguing that smoking pot makes you sexually violent, monstrous, out-of-control, and so on (the FBI built itself up from a nothing organization into what it is today based on this). Of course, it’s all nonsense and the legalization of cannabis has not resulted in any spikes in violence or crime—in fact, as with the end of prohibition, it has created some real losses for organized crime.
Cigarette butts are drug paraphernalia. Cigarette butts are a harm reduction tool. Cigarette butts are impossible to avoid. After the snow melts in winter, especially big messes of cigarette butts are revealed.
People who experience oppression, marginalization, criminalization, vulnerabilization, and vilification, are frequently discussed by the bureaucrats who are paid to manage them, the researchers who are paid to study them, and the social services who are funded to better them.
All of these people—the bureaucrats, researchers, and social service workers—operate under the more-or-less sincere belief that they approach the populations they manage, the cases they study, and the clients they support, in a caring manner.
Because of this, the people doing the talking are always coming up with new ways to talk about people that appear to be more sensitive or woke or humanizing, and less judgemental or derogatory. However, because the oppression, marginalization, criminalization, vulnerabilization, and vilification all continue despite the deployment of new labels, stigmas and biases then attach themselves to new seemingly-more-value-neutral terms. This cycle creates an ever-expanding market for new terms.
Folks like Peter Conrad and Joseph Schneider have tracked some of this in their explorations of how hegemonic social discourses moved from speaking about deviance to speaking in medical terms in the mid-to-late twentieth century. Things previously considered badness under the Christian morality that dominated Canadian society were rebranded as sickness in the post-Christian secular state. Thus, the immoral, vice-ridden sinner was rebranded as the “alcoholic” and the same became true of the “drug addict.”
The transition from the language of sin and vice to the language of addiction resonated a great deal with kind-hearted people who were trying to emphasize the human dignity and worth of the people they cared for and about. Instead of being a value judgment about a person’s character, addiction became a medical condition requiring the same kind of sensitive care and treatment as other medical conditions.
However, the medicalization of deviance was, simultaneously, the medicalization of social control. The transition from Christianity to secularism (ever-always an incomplete transition and one that may yet prove to be a temporary blip in Western statecraft) created a crisis for state power. Previously, Christian morality provided the moral underpinnings required to justify the use of force on the bodies of those who were considered problematical to the trajectory of the racial-capitalist state. The police, and other violence workers of the state, were justified in using force upon deviant bodies. After Christendom, the discursive apparatus of health replaced that of Christianity to justify forcing those considered deviant (now sick or ill or addicted) to do what they did not want to do, to go where they did not want to go, and to be where they did not want to be.
What vanishes from the now hegemonic dispositif of health is any kind of serious analysis of or engagement with oppression. Hence, also, its model of care lacks any truly liberatory praxis. I don’t want to overstate this—there is, of course, a continual process of subversion, co-optation, and hybridity (as per Homi Bhabha), taking place here. Nonetheless, it remains true that healthcare replaced Christianity as the moral discourse justifying the use of force on others, and the structures of oppression more generally, because it was more not less effective.
As a result, the same stigma began to accumulate around the language of “addiction” and “the addict” that had previously accreted around the terms used to describe “sinners,” “boozehounds,” and “junkies.” Consequently, “addiction” language quickly and easily became the discourse deployed by carceral Christianity and the forces of state violence.
As stated above (point #3), this inevitably occurs when people change their words but do not change their praxis. Social service organizations that have proven beneficial to maintaining the trajectory of the racial-capitalist status quo are particularly adept at constantly changing their language to reflect whatever cotemporary “evidence-based best practices” are trending—without modifying their polices, procedures, and actual practices in a meaningful way. Here, Gramsci’s notion of the “passive revolution” is relevant. Apparatuses are transformed due to pressure from below, but they are transformed in such a way that the power and priorities of the ruling classes are maintained or strengthened.
Research into the dynamics of what we call “addiction” have highlighted how much of our response to “addiction,” is unhelpful or even actively harmful. We now know that “the opposite of addiction is connection,” that harm reduction approaches are more successful than abstinence-based programs, and so on.
Therefore, instead of speaking about “drug addicts” or “drug addiction,” a lot of healthcare-oriented service providers began to use the language of “substance abuse.” This raises the odd philosophical question regarding if it is possible for a substance, like Adderall, to be “abused” but, more to the point, it still makes care-providers view the people they claim to care for as abusers. Consequently, healthcare providers now speak of “substance misuse” and “people who misuse substances.” They do this to try and avoid the not-so-subtle hint of moral condemnation that keeps creeping back into their language (because it turns out that a lot of what people thought was Christian morality is simply the bourgeois morality of racial capitalism).
Speaking of “people who misuse substances” raises the not-so-easily answered ethical question of what counts as the proper use of a substance and inevitably requires us to examine the power dynamics that determine who has the authority to decide what counts as use or misuse (the violence workers of the state? The doctors who prescribe medications under the law? people with lived and living experience?).
Is it misusing a substance to purchase and then smoke fentanyl because you have chronic pain and used to receive a prescription for Oxy-80s from your family doctor but now doctors will not prescribe narcotics like that for your pain and you have been flagged as “pill-seeking” because you continued to try and receive that medication (on which you now have a biochemical dependency—see point #18 below—which was created by a family doctor)?
More to the point raised above (see point #10), is it misusing a substance to take it to soothe your pain and briefly experience the kind of comfort, reprieve, and feelings of self-confidence or belovedness you have not been able to experience anywhere else? Perhaps there is a cost to seeking a reprieve via that substance… but does that mean I am misusing that substance? After all, most everything under the regime of racial capitalism comes at a cost to us (something sex workers have continually reminded us about when they have highlighted how sex work is work).
Therefore, care providers who are also more engaged with anti-oppressive practices (although see #7 above for how even this language is deployed in social services), have stopped using the language of “addiction” and instead speak of “self-soothing behaviours,” or “compulsively self-soothing behaviours.”
At this point, it’s important to observe that we all engage in self-soothing behaviours and do so, more-or-less compulsively, depending on what other supports and avenues we have to being adequately soothed by other people or a diverse number of things or activities.
To say that “the opposite of addiction is connection” is to highlight how much more compulsive our self-soothing becomes when we not only experience loneliness but are also abandoned by others—and most especially by those who should have cared for us or who explicitly profess to care for us (see point #2 above) but who fail to do so or who actively harm us instead.
To highlight this now is not to take away from the fact that biochemical dependencies can develop in very material, embodied ways, in relation to what we refer to as “addiction.” However, the language of “addiction” is selectively employed in such matters. I do not, for example, speak about being addicted to my anti-depressant, although a biochemical dependency exists in relation to this chemical intervention. I am urged to take my medication regularly to (amongst other things) avoid a painful, difficult, and mentally distressing withdrawal process; but people “who take drugs” are said to be addicts in the throes of addiction because they, too, seek to maintain regular doses of their meds. In my case, regular use is mandated by a doctor. In the second case, the use is said to be a compulsive craving. Often, it should be noted, for the very same chemical.
To this point, it is interesting when we speak of chemical interventions as “medications” and when we speak of them as “drugs” or, more generically, as “substances.” What often makes a chemical a “drug” instead of a “medication” is not the actual substance of the drug but whether it has been produced or acquired in a criminalized manner. For example, Adderall and Vyvanse, being virtually indistinguishable from crystal meth, are regularly acquired via both legal and criminalized channels. But if I get them from my doctor, I am taking medications. If I get them outside the Salvation Army, I am using drugs. Why are medications things that are “taken” but drugs are things that are “used”? I believe this subtle linguistic difference reveals a moral judgment.
Furthermore, the study of how our biochemistry changes in relation to our compulsive forms of self-soothing tends to focus almost entirely on matters related to chemically-induced forms of self-soothing and have less to say about other forms (although diet may be an exception—we know, for example, that our gut microbiome can learn to crave high-fat and high-sugar foods—foods regularly consumed as a form of self-soothing—so that we, ourselves, end up craving more and more food of that sort once we eat a certain amount of it because the bacteria in our gut craves those foods and tells us to crave it, too).
This is largely because some forms of compulsive self-soothing are socially accepted, sanctioned, and encouraged, while other forms are not. Workaholics, for example, are generally rewarded not only with wealth and power but also with high status. They accumulate both goods and goodness.
In 2000, The Onion published an editorial with the headline, “I’m Like A Chocoholic, But For Booze,” and this satire succeeds, like other brilliant forms of satire, because it reveals something true that we often overlook.
Whether or not a compulsive form of self-soothing is considered an “addiction,” has a lot to do with how that form of self-soothing impacts a person’s ability to function in ways that are deemed appropriate for them within the place they have inherited in racial capitalism.
In fact, our society has a high tolerance for compulsive forms of self-soothing that may cause problems for someone in their personal life, but which don’t interfere with that person’s ability to contribute to, or not interfere with, the trajectory of our status quo. Workaholics and Chocoholics have already been mentioned (points 21 and 22 above), but one can also think of people who compulsively watch pornography, or “wine moms,” or hardcore fitness freaks, or, more generally, our cultural dependence on caffeine (capitalism makes me wake-up feeling like shit… caffeine helps me perk up and makes me more functional as a wage-labourer).
Porn and alcohol are good examples that illustrate this point. Porn viewing, no matter how compulsive, is accepted if it doesn’t interfere with your work time and your ability to pay your bills. But if it interferes with those things, then it becomes an “addiction.” Same for drinking alcohol. Drink as much as you want, as long as you contribute to the system and don’t become dependent on the system. If you become dependent, well, now you’ve got a drinking problem.
This is also why the very same drugs, even when they are criminalized, are treated very differently depending on if people who hoard wealth or if impoverished people use them. Rich people take massive amounts of cocaine but, for the most part, this does not interfere with their ability to accumulate capital and advance the trajectory of the status quo. However, when impoverished people take the same amount of cocaine, this can genuinely disrupt their ability to work for wages, pay their bills, and accumulate credit-debt via the designated channels. Thus, the police focus on impoverished cocaine use and the rich are, by and large, left alone.
In other words, under racial capitalism, “substance misuse” or “addiction” more generally, is taken to be a form of compulsive self-soothing that interferes with one’s ability to perform the role one is expected to take in relation to one’s race, class, gender, ability, culture, and nationality.
More specifically, “addiction” and “substance misuse” are labels that are applied liberally to forms of compulsive self-soothing that transform a person into a real or potential obstacle to the smooth functioning of the trajectory of the status quo of racial capitalism.
This is part of the reason why, on the ground, people frequently choose to proudly claim labels that sensitive workers avoid. They recognize that the prettier sounding names that care providers give them are just masks covering the same old oppression. And so, just as feminists sometimes reclaim the “B” word and Black folks sometimes reclaim the “N” word, sometimes those whose medications or means of producing and procuring their medications have been criminalized, reclaim names like “junkie” or “crackhead,” or “waste case.”
Ultimately, this reminds us, liberation is less about labels and more about praxis. Which isn’t to say that words don’t matter—words, after all make worlds—but if the world that those words are making or remaking is the exact same world that abandoned us to die in the first place, well, that’s a problem that we can’t just talk our way out of.
In summary, the language of addiction (just like the language that came before and after it) is morally judgmental language deployed in an inconsistent, selective, and biased manner. It masquerades as a form of care but, in actual practice, further strengthens the hold of racial capitalism over our lives. But, just as the opposite of addiction is not abstinence but connection, so also the road to wellness is not recovery but liberation.
A good first step on that road to liberation is decriminalization. As the Adderall/crystal meth example reminds us (see point #19 above), most of the harms we try to reduce in relation to “street drugs,” are produced not by the substances themselves, but by criminalization. This has also been demonstrated in countries that have decriminalized drugs that are criminalized in Canada (Switzerland, Portugal), and it has also been demonstrated in innumerable studies, including several that have taken place in Canada.
The opposition to decriminalization, despite the overwhelming amount of evidence that supports it, reveals the extent to which “addiction science” and abstinence-based programs are still rooted in bourgeois Christian notions of “right” and “wrong.” The transition from “badness” to “sickness” (point #4 above), did not change anything fundamental about how oppressed people are treated, viewed by others, and made to feel about themselves. It did not change anything fundamental about how they are disciplined, punished, oppressed, and abandoned unto death.
This abandonment unto death is explicitly encouraged in abstinence-based programs that deliberately withdraw support from people so that they can “hit rock bottom.” For many people, rock bottom is six feet underground in a pauper’s grave. This is a vivid example of how the language of care is applied to death-dealing practices.
If our way of caring for people is killing them or exacerbating their suffering and contributing to them dying premature and preventable deaths, then we need to find other ways to care for people.
If I am trying to understand how to engage in a truly liberatory praxis, then I need to understand why I think the way I do about morality, about ethical issues, and about what I consider to be “right” and “wrong,” “okay” and “not okay.”
If I am trying to understand how to engage in a truly liberatory praxis, then I need to ask others (and myself!): What gives you life and affirms the life that is within you? What contributes to your sense of self-worth and belovedness? What eases your pain? What comforts you? What do you know that I don’t? (And what do I know that others don’t?) Where do you feel like you can relax? Where do you feel connection and belonging? Where do you feel at home? How have you been betrayed? What can I do that would make a meaningful difference to you? How can we get through this together?
Asking these questions doesn’t mean I cede my own agency to others. It doesn’t mean I just agree with everything that anyone says to me. It doesn’t mean that I refuse to set any boundaries. It just means that I come to others with a genuine openness, with a transparency about my own values and preconceived notions, with a willingness to learn and be transformed in ways that sometimes feel uncomfortable (or even wrong!) to me, with a faith in others and their abilities to identify their own areas of need, and with a genuine desire to be useful in ways that others identify as useful.
Note that this is very different than coming to people and saying, “You have (or are) a problem and I have (or am) the solution!” (The view expressed by countless White saviours and addiction workers.) The fact of the matter is that the oppression manufactured by and for racial capitalism is a problem for all of us. Mutually liberating solidarity—which is something we can only create together—is, in my opinion, the most hopeful way out of the mess that we all find ourselves in.
If this feels like I have drifted rather far from my thesis question (what do we talk about when we talk about “addiction”?), that’s kind of the point. Go and do likewise.